Fill Your Oklahoma Iep Form
Fill Your Oklahoma Iep Form
The Oklahoma Individualized Education Program (IEP) form serves as a crucial tool in the educational journey of children with disabilities, ensuring they receive the tailored support necessary for their unique needs. This comprehensive document begins with essential identifying information about the child, including their name, student ID, birthdate, and grade level. It also captures vital contact details for parents or guardians, allowing for effective communication throughout the IEP process. The form encompasses various sections that detail the child’s present levels of academic achievement and functional performance, highlighting how their disability impacts their learning and participation in the general education curriculum. Furthermore, it addresses the child's strengths and needs, taking into account special factors that may affect their education, such as behavioral interventions and communication requirements. The IEP outlines measurable annual goals, designed to foster academic and functional progress, alongside short-term objectives that provide a roadmap for achieving these goals. Transition planning is also a key component, especially for students approaching adulthood, as it prepares them for postsecondary education, employment, and independent living. Each section of the IEP emphasizes collaboration among educators, parents, and specialists, ensuring that the child’s educational experience is both enriching and supportive.
What Is an Apportioned Tag - Fill out the IRP Registration to comply with international vehicle registration standards.
In addition to its importance in the transfer of ownership, it's also essential for both parties to have access to reliable resources for completing the form correctly, such as those available at https://arizonapdfforms.com/motor-vehicle-bill-of-sale, which can provide guidance and templates for the Arizona Motor Vehicle Bill of Sale.
Free Oklahoma Child Custody Forms - It collects information on the child or children involved in the emergency custody situation.
What is the purpose of the Oklahoma IEP form?
The Oklahoma IEP form is designed to create a tailored educational plan for students with disabilities. It outlines the specific educational needs of the child and sets measurable goals to help them succeed in the general education curriculum. This form ensures that parents, educators, and specialists collaborate to support the child's academic and functional progress.
Who is involved in the IEP process?
The IEP process involves a team of individuals, including the child's parents, teachers, special education professionals, and any relevant specialists. This team collaborates to assess the child's needs, develop goals, and determine the necessary services and supports. The child may also be included in discussions, especially as they approach transition age.
How are goals measured in the IEP?
Goals in the IEP are measured through specific criteria set by the team. Each goal will have a method for tracking progress, such as regular assessments or reports. Parents will be informed of their child's progress throughout the year, ensuring they are aware of how their child is meeting or exceeding these goals.
What are the special factors considered in the IEP?
The IEP team considers several special factors that may impact the child's education. These include behavioral needs, language requirements for children with limited English proficiency, and the need for assistive technology. The team will check if these factors are relevant and explain any necessary services in the IEP.
When is the IEP reviewed and updated?
The IEP is reviewed at least once a year to assess the child's progress and make necessary adjustments. However, it can be amended more frequently if needed. Parents can request a review if they feel the child's needs have changed or if they have concerns about the current plan.
Completing the Oklahoma IEP form involves several important steps to ensure that all necessary information is accurately captured. Following these steps will help in creating a comprehensive plan tailored to the child's educational needs.
After completing these steps, review the form for accuracy. Ensure that all sections are filled out thoroughly. This will help in developing a clear and effective IEP that addresses the child's unique educational needs.
The Oklahoma Individualized Education Program (IEP) form shares similarities with the 504 Plan, which is designed to provide accommodations and modifications for students with disabilities. Both documents aim to ensure that students have equal access to education. The IEP focuses on special education services tailored to the individual needs of the child, while the 504 Plan outlines necessary adjustments within the general education setting. Both require input from parents and educational professionals to create a supportive environment for the student.
Another document that resembles the Oklahoma IEP form is the Individual Family Service Plan (IFSP). The IFSP is specifically designed for infants and toddlers with developmental delays. Like the IEP, it includes information about the child's strengths and needs, as well as specific goals and services required. However, the IFSP emphasizes family involvement and support, recognizing the family's role in the child's development, whereas the IEP focuses more on the educational setting and outcomes for school-age children.
The Personalized Learning Plan (PLP) also shares characteristics with the Oklahoma IEP. A PLP is typically used to customize a student's learning experience based on their unique strengths and interests. Both documents outline goals and strategies for achieving educational success. However, while the IEP is a legal document with specific requirements under federal law, the PLP is often more flexible and may not have the same legal implications, allowing for a more individualized approach to learning.
In addition, the Behavior Intervention Plan (BIP) is similar to the IEP in that it addresses specific needs related to a child's behavior. Both documents are developed collaboratively by a team that may include parents, educators, and specialists. The BIP focuses on strategies to improve behavior and ensure that the child can participate in the educational environment effectively. The IEP may incorporate elements of the BIP if behavioral issues impact the child's learning and progress.
For individuals looking to enhance their understanding of legal documents related to asset transactions, resources are available to assist you, such as the information found at legalpdf.org, which can guide you through the process of creating a Bill of Sale and ensuring all necessary details are accurately documented.
Lastly, the Transition Plan is another document that aligns with the Oklahoma IEP. This plan is often part of the IEP for students approaching adulthood and focuses on preparing them for life after high school. Both documents outline goals and services needed for successful transitions, whether into further education, employment, or independent living. The Transition Plan emphasizes the importance of planning for the future, while the IEP ensures that the student receives the necessary support throughout their educational journey.
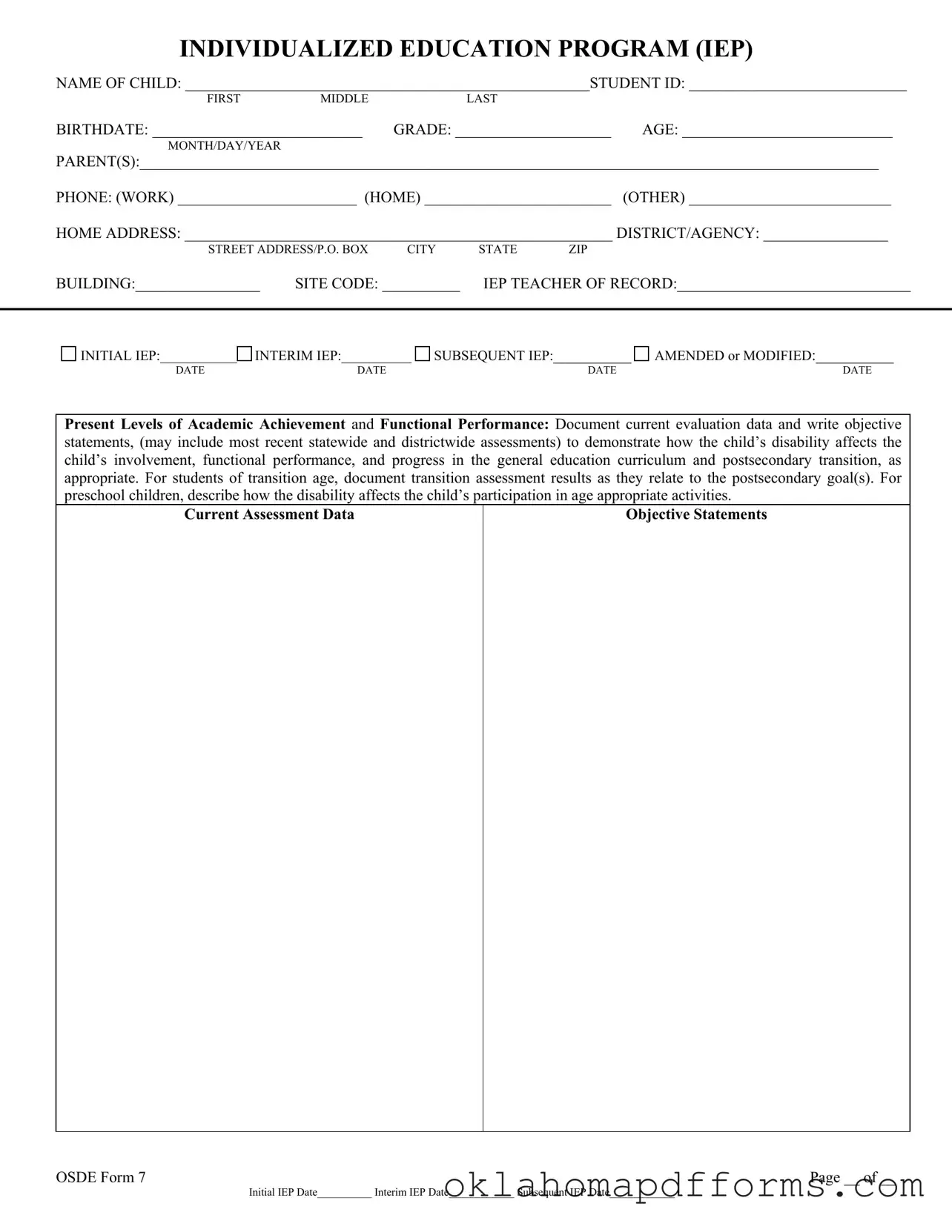
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
NAME OF CHILD: ____________________________________________________STUDENT ID: ____________________________
FIRST MIDDLELAST
BIRTHDATE: ___________________________ |
GRADE: ____________________ |
AGE: ___________________________ |
|||
MONTH/DAY/YEAR |
|
|
|
|
|
PARENT(S):_______________________________________________________________________________________________ |
|||||
PHONE: (WORK) _______________________ (HOME) ________________________ |
(OTHER) __________________________ |
||||
HOME ADDRESS: _______________________________________________________ DISTRICT/AGENCY: ________________ |
|||||
STREET ADDRESS/P.O. BOX |
CITY |
STATE |
ZIP |
|
|
BUILDING:________________ |
SITE CODE: __________ |
IEP TEACHER OF RECORD:______________________________ |
|||
|
|
|
|
|
|
INITIAL IEP:___________ |
INTERIM IEP:__________ |
SUBSEQUENT IEP:__________ |
DATE |
DATE |
DATE |
AMENDED or MODIFIED:__________
DATE
Present Levels of Academic Achievement and Functional Performance: Document current evaluation data and write objective statements, (may include most recent statewide and districtwide assessments) to demonstrate how the child’s disability affects the child’s involvement, functional performance, and progress in the general education curriculum and postsecondary transition, as appropriate. For students of transition age, document transition assessment results as they relate to the postsecondary goal(s). For preschool children, describe how the disability affects the child’s participation in age appropriate activities.
Current Assessment Data
Objective Statements
OSDE Form 7 |
Page __ of __ |
|
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________ |
IEP – Strengths/Needs, Special Factors, and Parent Concerns Page
List strengths of the child and a statement of the anticipated |
List the educational needs resulting from the child’s disability, |
effects on the child’s participation in the general education |
which may require special education, related services, |
curriculum or appropriate activities. |
supplementary aids, supports for personnel, or modifications. |
|
|
Strengths: |
|
Anticipated Effects:
Consideration of special factors: Check yes or no whether the IEP team considers each special factor to be relevant to this child. Yes No
Strategies, positive behavior interventions and supports, as appropriate, if behavior impedes learning of self or others
Language needs as related to the IEP for a child with limited English proficiency (LEP)
Instruction and use of Braille if child is blind or visually impaired, unless determined inappropriate based on evaluation.
Communication needs, and for child who is deaf or hard of hearing, the language and communication needs and opportunities for communication and instruction in the child’s native language and communication mode
Whether this child requires assistive technology devices and service
For special factors checked yes, explain determinations of the team as to whether services are required in the IEP.
Parent Concerns for Enhancing the Child’s Education:
OSDE Form 7 |
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
IEP – Goals Page
NAME OF CHILD: |
|
|
|
STUDENT ID:_________________________ |
|
FIRST |
MIDDLE |
LAST |
|
Annual Goals:
Provide measurable annual goals, including academic and functional goals to enable the child to be involved in and make progress in the general education curriculum (for a preschool child in the appropriate activities), and to meet other educational needs that result from the disability.
GOAL # _______
Parents are to be informed of progress in annual goals, in addition to general education academic performance reports. Describe how often this will occur and what methods will be utilized.
Record the extent of progress toward achieving the annual goals by the end of the year (i.e.,
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
How will the extent of progress toward annual goals be measured?
GOAL # _______
Parents are to be informed of progress in annual goals, in addition to general education academic performance reports. Describe how often this will occur and what methods will be utilized.
Record the extent of progress toward achieving the annual goals by the end of the year (i.e.,
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
How will the extent of progress toward annual goals be measured?
GOAL # _______
Parents are to be informed of progress in annual goals, in addition to general education academic performance reports. Describe how often this will occur and what methods will be utilized.
Record the extent of progress toward achieving the annual goals by the end of the year (i.e.,
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
How will the extent of progress toward annual goals be measured?
COMMENTS:
OSDE Form 7 |
|
Page __ of __ |
|
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________ |
|
|
|
IEP – Goals and
NAME OF CHILD: |
|
|
|
STUDENT ID:_________________________ |
|
FIRST |
MIDDLE |
LAST |
|
Annual Goals:
Provide measurable annual goals, including academic and functional goals to enable the child to be involved in and make progress in the general education curriculum (for a preschool child in the appropriate activities), and to meet other educational needs that result from the disability.
GOAL # _______
Parents are to be informed of progress in annual goals, in addition to general education academic performance reports. Describe how often this will occur and what methods will be utilized.
Record the extent of progress toward achieving the annual goals by the end of the year (i.e.,
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
How will the extent of progress toward annual goals be measured?
COMMENTS:
OSDE Form 7 |
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
IEP – Transition Services Plan – Goals and Activities Page
(Beginning not later than the first IEP developed during the student’s ninth grade year, or upon turning 16 years of age, whichever occurs first)
NAME OF CHILD: |
|
|
|
STUDENT ID: ________________________ |
|
FIRST |
MIDDLE |
LAST |
|
Postsecondary Goal(s): _________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Annual Transition Goals
Provide measurable annual transition goals to assist the young adult in working toward their postsecondary goal(s). The annual transition goal(s) must include academic and functional goals to enable the young adult to be involved in and make progress in the general education curriculum and in community experiences. For a young adult beginning with the first IEP developed during the student’s ninth grade year or upon turning 16 years of age, whichever occurs first, postsecondary goal(s) based upon age appropriate transition assessments related to education/training, employment, and where appropriate, independent living skills, and to meet other educational needs that result from the disability. For young adults being taught to alternate achievement of the standards, include a minimum of two (2)
Education/Training Goal(s) |
||||||
|
|
|
|
|
|
|
Coordinated Activities |
Responsible Party(ies) |
|
|
|
||
|
|
|
|
|
|
|
Parents are to be informed of progress in annual goals, in addition to general |
Extent of progress toward achieving the annual transition goals by |
|||||
education academic performance reports. Describe how often this will occur |
the end of the year (i.e., |
|||||
and what methods will be utilized. |
grades in general curriculum). |
|
|
|
||
|
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
How will the extent of progress toward annual goals be measured? |
|
|
|
|
|
|
|
|
|
|
|
|
|
Employment Goal(s) |
||||||
|
|
|
|
|
|
|
Coordinated Activities |
Responsible Party(ies) |
|
|
|
||
|
|
|
|
|||
Parents are to be informed of progress in annual goals, in addition to general |
Extent of progress toward achieving the annual transition goals by |
|||||
education academic performance reports. Describe how often this will occur |
the end of the year (i.e., |
|||||
and what methods will be utilized. |
grades in general curriculum). |
|
|
|
||
|
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
How will the extent of progress toward annual goals be measured? |
|
|
|
|
|
|
|
|
|
|
|
|
|
OSDE Form 7 |
|
|
|
|
|
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
IEP – Transition Services Plan – Transition Goals/Course of Study
(Beginning not later than the first IEP developed during the student’s ninth grade year or upon turning 16 years of age, whichever occurs first.)
NAME OF CHILD: |
|
|
|
|
STUDENT ID:_________________________ |
|||||
|
FIRST |
MIDDLE |
LAST |
|
|
|
|
|
|
|
Independent Living Goal(s) (if appropriate) |
|
|
||||||||
|
|
|
|
|
|
|
|
|
||
Coordinated Activities |
|
|
Responsible Party(ies) |
|
|
|
||||
|
|
|
|
|
|
|
|
|||
Parents are to be informed of progress in annual goals, in addition to general |
|
Extent of progress toward achieving the annual transition goals by |
||||||||
education academic performance reports. Describe how often this will occur |
|
the end of the year (i.e., |
||||||||
and what methods will be utilized. |
|
|
grades in general curriculum). |
|
|
|
||||
|
|
|
|
DATE |
DATE |
DATE |
DATE |
DATE |
DATE (ESY) |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
How will the extent of progress toward annual goals be measured? |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Build a course of study, to be updated annually, to assist the young adult in achieving their postsecondary goal(s):
Grade __________ |
Grade __________ |
Grade __________ |
Grade __________ |
Grade ___________ |
Projected date of graduation/program completion and type:
______________________________________
______________________________________
Standard Diploma
General Education Development (GED) Other _____________________________
In planning the course of study, is information needed regarding opportunities for vocational education (e.g., high school vocational education courses,
Yes No
If yes, document date(s) when information was provided to young adult and parent(s). Date: ______________________
By age 16, the young adult has been referred to the vocational rehabilitation counselor in the young adult’s school district.
Yes No
Person responsible for the referral: __________________________________________Date:__________________________________
Name of the Vocational Rehabilitation Counselor: ____________________________________________________________________
Have the young adult and parent(s) been provided a copy of the referral form? Yes No
If no, explain why. _____________________________________________________________________________________________
If yes, explain how. ____________________________________________________________________________________________
By age 17, have young adult and parent(s) been informed of any transfer of rights at age of majority? Yes No
If no explain why: _____________________________________________________________________________________________
Comments: __________________________________________________________________________________
OSDE Form 7 |
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
IEP – Services Page
NAME OF CHILD: |
|
|
|
|
|
STUDENT ID:_________________________ |
||||
|
FIRST |
|
MIDDLE |
LAST |
|
|
|
|
||
|
|
|
|
|
|
|
||||
Special Education Services: List each special education service. |
|
|
|
|
||||||
Type of Service(s) |
|
|
Amount of Services (Time |
Starting Date |
Ending Date |
Person Responsible |
||||
|
|
|
|
|
|
and Frequency) |
|
|
|
(Title) |
|
|
|
|
|
|
|||||
Related Services: List each related service necessary for the child to benefit from special education. |
|
|||||||||
Type of Service(s) |
|
Location of |
|
Amount of Services (Time |
Starting Date |
Ending Date |
Person Responsible |
|||
|
|
|
Services |
|
|
and Frequency) |
|
|
|
(Title) |
|
|
|
|
|
|
|
|
|
|
|
Provide an explanation of the extent, if any, to which the child will not participate with nondisabled children in the general education curriculum or
The continuum of placements for the least restrictive environment (LRE) includes regular classes
Continuum of Placement:
Amount of time in general education setting: _____ of _____ periods per day OR __________ % of instructional day.
If block schedule, describe:
Is this child’s instructional day the same length as nondisabled peers? Yes No
If no, describe the reason(s) for a shortened school day:
Regular PE Adapted PE NA |
List modifications necessary for this child to participate in regular PE |
If not applicable provide justification: |
(specially designed adapted PE, if needed, must be addressed on the IEP): |
|
|
|
|
Supplementary aids and services, program modifications and/or supports for personnel in general education or other
Supplementary aids and services: |
Location/Class/Settings |
|
|
Program modifications: |
Location/Class/Settings |
|
|
Supports for personnel: |
Location/Class/Settings |
|
|
OSDE Form 7 |
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
IEP – Signature Page
NAME OF CHILD: |
|
|
|
STUDENT ID:_________________________ |
|
|
FIRST |
MIDDLE |
LAST |
|
|
State and Districtwide Assessment Programs |
|
|
|
||
Child will participate in: |
Oklahoma Core Curriculum Tests (OCCT) |
Alternate Assessment (OAAP or OMAAP) |
|||
If the child is participating in alternate assessment, has the IEP team considered the guidelines for participation in alternate assessment?
Yes No If no, explain why: |
|
|
If the child is participating in an alternate assessment, how will the child be assessed? |
OAAP Portfolio |
OMAAP |
If the child is participating in OMAAP, list each subject for which the child will participate. |
|
|
Specify state approved accommodations used in each test administration. |
|
|
Extended School Year (ESY) Services
ESY Services: Requires further data; will reconvene by ___/____/___ |
are necessary |
are not necessary |
If necessary, describe services provided: |
|
|
Documentation of LRE Placement Considerations
Describe continuum of placements considered and reasons determined not appropriate:
Is this placement in the school the child would normally attend if nondisabled? Yes No
If no, is the placement as close as possible to the child’s home? Yes No
If no, explain why the IEP requires other arrangements:
Explain considerations of potential harmful effects on the child or the quality of services needed:
When special classes, separate schools/facilities, or other removal from the general education environment occurs, describe how the nature and severity of the disability is such that education in general education classes, with the use of supplementary aids and services, cannot be achieved satisfactorily:
Date of next IEP _______________________________________________________________Date of next 3 year reevaluation ______________
FROM INITIAL |
FROM INTERIM |
FROM SUBSEQUENT |
|
|
|
Team Participant Signatures: |
|
|
|
|
|
Parent(s)________________________________________________ |
Date _________________ |
Agree |
*Disagree |
||
Special Education Teacher__________________________________ |
Date _________________ |
Agree |
*Disagree |
||
Regular Education Teacher _________________________________ |
Date _________________ |
Agree |
*Disagree |
||
Administrative Representative_______________________________ |
Date _________________ |
Agree |
*Disagree |
||
Student _________________________________________________ |
Date _________________ |
Agree |
*Disagree |
||
Other___________________________________________________ |
Date _________________ |
Agree |
*Disagree |
||
*Team members who disagree may submit separate statements presenting their conclusions. (Complete Comment Form as necessary.)
If parent(s) did not attend the IEP meeting, explain other methods to ensure parent participation (and/or child as appropriate): (e.g., conference call, videoconference, home visit)
Parent(s) have protection under the procedural safeguards. |
Translation/Interpretation needed: |
Yes No |
|
Parent(s) received Parents Rights in Special Education: |
If yes, specify how provided: ______________________ |
||
Notice of Procedural Safeguards |
|
|
|
Yes |
No |
|
|
Parent(s) received Parent Survey form and business reply envelope: |
Parent Initial: _____________________ |
||
Yes |
No |
|
|
Parent consent for initial placement (consent is voluntary and may be revoked at any time) |
Yes No |
||
Parent Signature: _______________________________________________________ Date: _________________________________
OSDE Form 7 |
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
OSDE Form 7 |
Page __ of __ |
Initial IEP Date__________ Interim IEP Date____________ Subsequent IEP Date____________
The Oklahoma IEP form is a crucial document in the educational planning process for children with disabilities. Alongside this form, several other documents are commonly used to ensure a comprehensive approach to meeting the educational needs of the child. Below is a list of these additional forms and documents, each serving a specific purpose in the development and implementation of an Individualized Education Program.
These documents work together to create a comprehensive framework for supporting the educational journey of children with disabilities. Each plays a vital role in ensuring that the child's individual needs are met and that parents are actively involved in the process.
Start by gathering all necessary information about the child, including their name, student ID, and birthdate. This foundational data is essential for accurately filling out the IEP form.
Document the child’s current academic performance and functional capabilities. This section should highlight how the child's disability impacts their learning and participation in the general education curriculum.
Clearly outline the child’s strengths and needs. Identifying these aspects helps the IEP team develop effective strategies tailored to support the child’s educational journey.
Set measurable annual goals that encompass both academic and functional objectives. These goals should aim to enhance the child’s involvement in the general education curriculum.
For each annual goal, include at least two short-term objectives or benchmarks. These smaller milestones will guide progress and help track achievements throughout the year.
Consider special factors that may affect the child’s learning. This includes behavioral strategies, language needs, and any assistive technology requirements that could support the child’s education.
Maintain open communication with parents regarding their child’s progress. Regular updates about the child’s advancement towards annual goals are crucial for fostering a collaborative environment.